Skin Infections Confirmed as a Cause of Acute Rheumatic Fever
By LabMedica International staff writers
Posted on 05 Jan 2022
Infection with group A streptococcus (GAS) can trigger an immune-mediated response in a small minority of people, resulting in acute rheumatic fever (ARF). ARF produces an inequitable burden of disease, with the highest rates in low and middle-income countries and among some, often indigenous-minority populations living in high-income countries.Posted on 05 Jan 2022
Group A Streptococcus (GAS; Streptococcus pyogenes) is a bacterium which can colonize the throat, skin and anogenital tract. It causes a diverse range of skin, soft tissue and respiratory tract infections. GAS can occasionally cause infections that are extremely severe. Invasive GAS (iGAS) is an infection where the bacteria is isolated from a normally sterile body site, such as the blood.
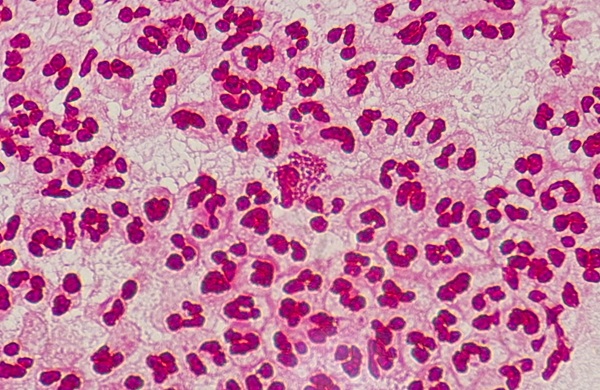
 illustration depicts four, yellow colored, Group A Streptococcus (GAS), Streptococcus pyogenes bacteria (Photo courtesy of National Institute of Allergy and Infectious Diseases)")
Image: Digitally colorized scanning electron microscopic (SEM) illustration depicts four, yellow colored, Group A Streptococcus (GAS), Streptococcus pyogenes bacteria (Photo courtesy of National Institute of Allergy and Infectious Diseases)
Infectious disease specialists at the University of Otago Wellington (Wellington, New Zealand) and their colleagues carried out a retrospective analysis used pre-existing administrative data. Throat and skin swab data (1,866,981 swabs) from the Auckland region, New Zealand and antibiotic dispensing data were used (2010–2017). Incident ARF cases were identified using hospitalization data (2010–2018). The risk ratio (RR) of ARF following swab collection was estimated across selected features and timeframes. Antibiotic dispensing data were linked to investigate whether this altered ARF risk following GAS detection.
Swabs were cultured onto tryptic soy sheep blood agar and incubated for 48 hours at 37 °C in 5% CO2. Plates were reviewed after 24 and 48 hours of incubation, and colonies indicating beta-hemolytic streptococci were identified. Prior to 2012, streptococcal grouping latex was used to identify beta-hemolytic streptococci. From 2012 onwards, MALDI-TOF MS Biotyper (Bruker, Karlsruhe, Germany) was used. Emm-typing for GAS strain identification is not used in routine diagnostic testing, so strain-typing data were unavailable.
The investigators reported that ARF risk increased following GAS detection in a throat or skin swab. Māori and Pacific Peoples had the highest ARF risk 8–90 days following a GAS-positive throat or skin swab, compared with a GAS-negative swab. During this period, the RR for Māori and Pacific Peoples following a GAS-positive throat swab was 4.8 and following a GAS-positive skin swab, the RR was 5.1. Antibiotic dispensing was not associated with a reduction in ARF risk following GAS detection in a throat swab (antibiotics not dispensed (RR: 4.1), antibiotics dispensed (RR: 4.3), or in a skin swab (antibiotics not dispensed (RR: 3.5), antibiotics dispensed (RR: 2.0).
Michael Baker, MBChB, FNZCPHM, FAFPHM, FRACMA, DComH, DObst, a Professor of Public Health and a senior author of the study, said, “This study is a major breakthrough in understanding the causes of acute rheumatic fever. It is the world’s first study to confirm that the risk of rheumatic fever rises after a GAS skin infection in a similar way to how it does after a GAS sore throat. Because acute rheumatic fever is an uncommon disease and few countries have comprehensive linked health data, no previous study has been able to quantify the rheumatic fever risk following a laboratory-confirmed infection.”
The authors concluded that prompt antibiotic treatment of GAS infections in groups with a known high risk of ARF is required to terminate the infective process, reducing the risk of poor outcomes, and to limit GAS transmission. Targeted sore throat management interventions should remain a key strategy in the prevention of ARF. The study was published on December 9, 2021 in the journal BMJ Global Health.
Related Links:
University of Otago Wellington
Bruker
Gold Member
Flocked Fiber Swabs
Puritan® Patented HydraFlock®


Clinical Informatics Platform
CLARION™
Hematology Consumables
Bioblood Devices