Mismatch Repair/Microsatellite Instability Evaluated Using Cytology Effusion Specimens
By LabMedica International staff writers
Posted on 25 Jan 2021
DNA mismatch repair (MMR) status is routinely assessed in colorectal and endometrial carcinoma as a method of cancer prevention, surveillance in patients with Lynch syndrome and their families, and for prognostic, predictive, and therapeutic implications. Posted on 25 Jan 2021
MMR is a highly conserved process involving the four key genes mutL homologue 1 (MLH1), mutS homologue 2 (MSH2), mutS homologue 6 (MSH6), and postmeiotic segregation increased 2 (PMS2), which act to identify and repair mismatched base pairs that may arise during DNA replication. Recent studies have shown that patients with microsatellite instability-high (MSI-H) or mismatch repair–deficient (dMMR) advanced cancers can benefit from treatment with a immune checkpoint inhibitor.
 (Photo courtesy of Leica Biosystems).")
Image: The Leica Bond III stainer is fully automated Immunohistochemical and In Situ Hybridization (IHC and ISH stainer) (Photo courtesy of Leica Biosystems).
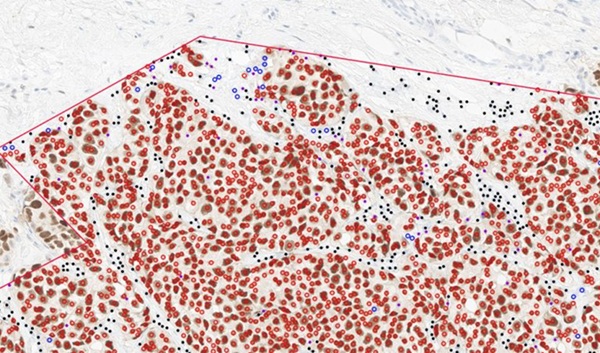
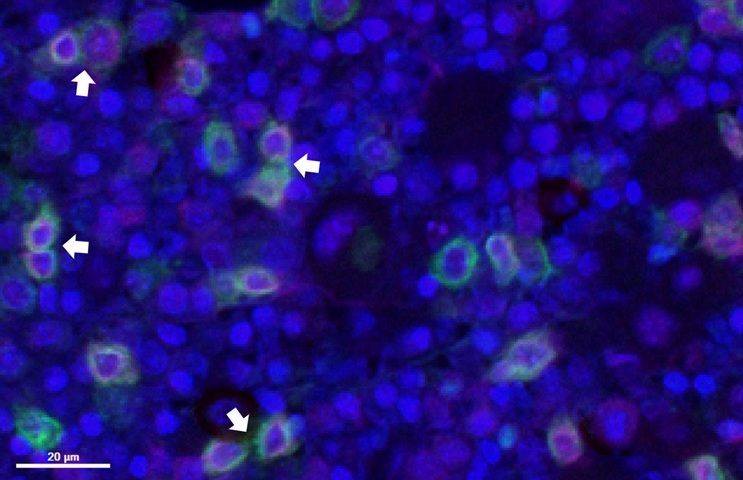
Medical Scientists at The University of Texas MD Anderson Cancer Center (Houston, TX, USA) identified surgical pathology cases of colorectal and endometrial carcinomas with known MMR/MSI status and matched effusions with available cell blocks (CBs). Cell block sections were evaluated for adequacy and stained with MMR IPOX (MSH2, MSH6, MLH1, and PMS2). Cytological effusion specimens were collected at the institution by using standard techniques, received fresh in the cytology laboratory, and processed within 48 hours and a cell block was prepared according to previously described techniques and a laboratory protocol.
Immunoperoxidase staining for MLH1, PMS2, MSH2, and MSH6 was performed on unstained CB sections with the Leica Bond III stainer (Leica Biosystems, Buffalo Grove, IL, USA). The team identified 748 cases with MMR/MSI testing on surgical specimens having matched effusions. Of these, 131 cases (17.5%) had an available CB and 53 were deemed adequate for MMR IPOX staining. MMR IPOX results between effusion CBs and surgical pathology specimens were concordant in 45 of 53 (85%), inconclusive in six of 53 (11%), and discordant in two of 53 (4%) cases.
The authors concluded that there was high concordance of MMR IPOX testing between cytological and surgical specimens, with no false-positive and only two false-negative CB results. Limited tumor cells, staining in cells indefinite as tumor, tumor staining heterogeneity, and lack of internal control staining were problematic in some cases. Their findings indicate that cytological effusion specimens may be suitable substrates for MMR IPOX biomarker testing; however, inconclusive cases need to be interpreted with caution. The study was published in the January 2021 issue of the journal Archives of Pathology and Laboratory Medicine.
Related Links:
The University of Texas MD Anderson Cancer Center
Leica Biosystems

Gold Member
Automatic Hematology Analyzer
CF9600


Pipette Calibration System
Artel PCS®

Clinical Informatics Platform
CLARION™