Liquid Biopsy Identifies Advanced Lung Cancer Drivers
By LabMedica International staff writers
Posted on 13 Dec 2018
Liquid biopsy for plasma circulating tumor DNA (ctDNA) next-generation sequencing (NGS) is commercially available and increasingly adopted in clinical practice despite a paucity of prospective data to support its use.Posted on 13 Dec 2018
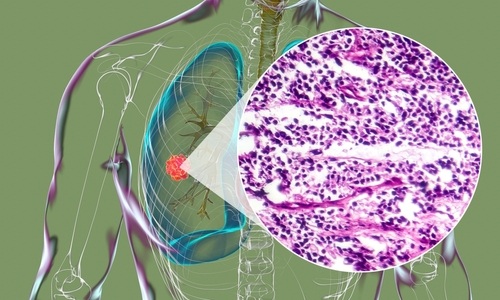
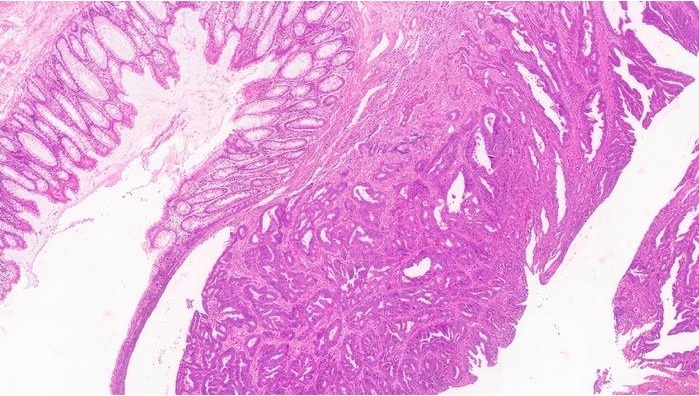
Plasma ctDNA harboring somatic mutations are highly specific for cancer and may serve as a useful surrogate of tumor burden, intratumor heterogeneity, and response to therapy. Genetic sequencing is particularly important in patients with advanced-stage non-small cell lung cancers as their tumors may harbor somatic alterations that are sensitized to targeted therapies.
 next-generation sequencing (NGS) assay (Photo courtesy of ArcherDx).")
Image: The Rapid Amplification of ctDNA Ends (RACE) next-generation sequencing (NGS) assay (Photo courtesy of ArcherDx).
A large international team of scientists collaborating with the Memorial Sloan Kettering Cancer Center (New York, NY, USA) enrolled a total of 210 consecutive patients with advanced non-small cell lung cancer, and the majority of patients had adenocarcinoma histology (192/210, 91.4%). Patients were predominantly female (124/210, 59.0%). All patients had metastatic disease at the time of plasma NGS genotyping. Most patients (171/210, 81.4%) had prior conventional molecular tumor testing (immunohistochemistry, PCR fluorescence in situ hybridization for EGFR, ALK, and ROS1) performed and resulted on tissue at the time of plasma NGS testing.
For 106 of the cases, they also had access to targeted NGS data across 468 cancer-related genes, generated on tumor tissue biopsy samples analyzed with the Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets (MSK-IMPACT) capture assay. Sufficient tumor tissue was not available for molecular testing in 39 of the cases. A subset of patients who had an alteration identified on ResBio plasma ctDNA NGS underwent orthogonal plasma testing with an anchored multiplex PCR assay based on Rapid Amplification of ctDNA Ends (RACE) strategy. Additionally, the team assessed a subset of the blood plasma samples with an Archer RACE NGS assay to verify the accuracy of the ctDNA findings.
The team detected somatic mutations in 64.3% (135/210) of patients. Circulating tumor DNA detection was lower in patients who were on systemic therapy at the time of plasma collection compared with those who were not (30/70, 42.9% versus 105/140, 75.0%). The median test turnaround time (TAT) of plasma NGS was shorter than tissue NGS (9 versus 20 days). Patients who tested plasma NGS positive for oncogenic drivers had tissue NGS concordance of 96.1% (49/51) and directly led to matched targeted therapy in 21.9% (46/210) with clinical response.
The authors concluded that plasma ctDNA NGS detected a variety of oncogenic drivers with a shorter TAT compared with tissue NGS and matched patients to targeted therapy with clinical response. Positive findings on plasma NGS were highly concordant with tissue NGS and can guide immediate therapy; however, a negative finding in plasma requires further testing. The study was published on November 28, 2018, in the Journal of the National Cancer Institute.
Related Links:
Memorial Sloan Kettering Cancer Center
Gold Member
Quantitative POC Immunoassay Analyzer
EASY READER+


Chromogenic Culture System
InTray™ COLOREX™ ECC

Multi-Chamber Washer-Disinfector
WD 390