Human Granulocytic Anaplasmosis Confirmed by Molecular Assay
By LabMedica International staff writers
Posted on 26 Mar 2012
Human granulocytic anaplasmosis (HGA) is a tick-borne infection, yet few clinical cases have been diagnosed by a positive polymerase chain reaction (PCR) assay. Posted on 26 Mar 2012
Subsequent seroconversion against the antigen of the causative intraerythrocytic agent, Anaplasma phagocytophilum, would fulfill the epidemiologic, clinical, and biological criteria for HGA, which is characterized by an acute, nonspecific febrile illness.
.")
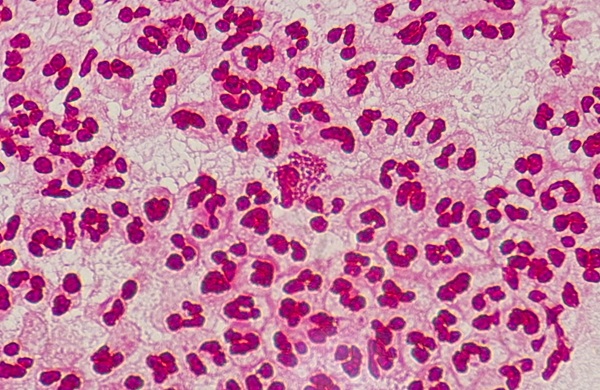
Image: Anaplasma phagocytophilum, causative agent for anaplasmosis (Photo courtesy of Medscape).
At the Hôpitaux Universitaires de Strasbourg (France), 15 patients presented with a febrile syndrome with a recent history of tick bites or exposures to ticks were tested for HGA, during the period June to September 2009. Whole blood samples with ethylenediaminetetraacetic acid (EDTA) were systematically collected for blood smear and specific PCR assay during the febrile phase of the disease. For serologic testing, two sera were also collected: the first during the acute phase and the second two to three weeks afterwards, during the convalescent phase.
DNA was extracted from whole-blood samples and real-time PCR was performed on the ABI Prism 7000 SDS (Applied Biosystems; Foster City, CA, USA). Serologic diagnosis of infection with A. phagocytophilum was made by immunofluorescent antibody test (IFA) (Focus Diagnostics, Cypress, CA, USA). Serum specimens with immunoglobulin M (IgM) titers of equal or greater than 1:40 and IgG titers equal to or greater than 1:64 were considered positive. Blood smears were obtained from whole blood samples, stained with May-Grünwald-Giemsa and examined for the presence of morulae within the cytoplasm of neutrophils
Molecular testing using the major surface protein 2 (msp2)/p44 gene yielded positive results in the acute-phase blood of three of the 15 patients tested. For the 12 patients with negative PCR assay, microscopic examination was negative and no specific antibodies were detected in acute-phase serum. Laboratory findings were available for 6 patients among the 12 with a negative PCR assay; all these 6 presented leucopenia, thrombocytopenia, and increased levels of liver enzymes. For the three patients with positive PCR results, examination of peripheral blood smears revealed cytoplasmic inclusions suggestive of A. phagocytophilum morulae and elevated serum levels of liver enzymes.
The authors concluded that a specific PCR assay on EDTA anticoagulated blood may be the diagnostic test of choice for HGA during the first two weeks following the onset of symptoms, allowing a faster diagnosis than serology. HGA should be included in the differential diagnosis of patients presenting febrile illness associated with bicytopenia, elevated rates of liver enzymes, increased C-reactive protein values, and whose medical history reveals recent exposure to ticks. The study was published in the March 2012 issue of the journal Diagnostic Microbiology and Infectious Disease.
Related Links:
Hôpitaux Universitaires de Strasbourg
Applied Biosystems
Focus Diagnostics

New
Gold Member
POC Helicobacter Pylori Test Kit
Hepy Urease Test


New
Fully-auto Specific Protein (Nephelometry) Analyzer
PA240

Steam Sterilizer
Hi Vac II Line