Confirmation Testing for Primary Hyperaldosteronism Remains Essential
By LabMedica International staff writers
Posted on 10 Jul 2019
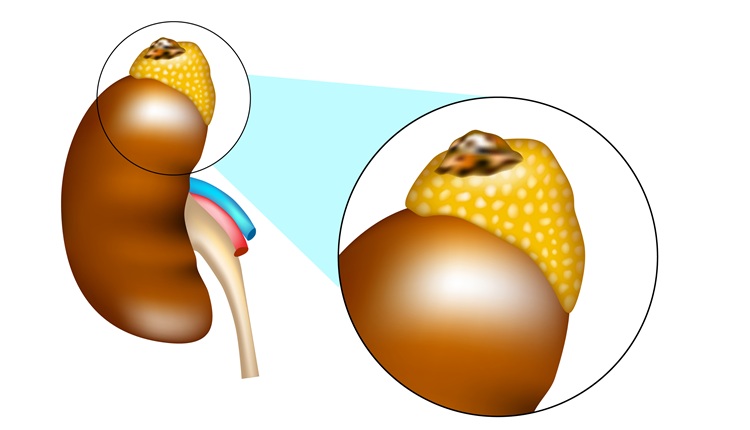
Primary aldosteronism, also known as primary hyperaldosteronism (PHA) or Conn's syndrome, refers to the excess production of the hormone aldosterone from the adrenal glands, resulting in low renin levels. This abnormality is caused by hyperplasia or tumors.Posted on 10 Jul 2019
Primary hyperaldosteronism is among the most common causes of secondary hypertension, with a prevalence of ~4.3% in patients with hypertension. Many suffer from fatigue, potassium deficiency and high blood pressure, which may cause poor vision, confusion or headaches. Symptoms may also include: muscular aches and weakness, muscle spasms, low back and flank pain from the kidneys, trembling, tingling sensations, numbness and excessive urination.
Scientists working with the University Hospital Olomouc and Palacký University (Olomouc, Czech Republic) performed confirmatory testing on 312 ambulatory patients with severe or resistant arterial hypertension who had an aldosterone-to-renin ratio (ARR) of >30 or aldosterone levels of >150 ng/L. The confirmatory testing was performed with identical laboratory examinations before and after infusion of saline for four hours and after withdrawal of potentially interfering medications.
Patients with confirmed PHA were more likely to be men (70.3% versus 54.9%), had lower serum potassium (3.8 versus 4.1 mmol/L) and plasma renin activity (0.7 versus 3.2), higher serum aldosterone (268 versus 229 ng/L) and ARR (177 versus 95), higher office systolic blood pressure (147 versus 143 mmHg). Significant predictors of PHA were plasma renin assay (PRA) < 0.63 (AUC ROC 0.63), aldosterone >165 ng/L (AUC 0.60), ARR > 43 (AUC 0.68), serum potassium <4.0 mmol/L (AUC 0.68) and the number of used antihypertensive drugs >4 (AUC 0.64).
When applied to the cohort, combined recommended cut-off values determined by international guidelines that further testing was not needed (aldosterone >200 ng/L and potassium <4.0 mmol/L) had an overall accuracy for diagnosis of primary hyperaldosteronism of only 69.0%. A combination of ARR >43 and serum potassium <4 mmol/L had overall accuracy for primary hyperaldosteronism of 75.6%.
Jan Vaclavik, MD, the senior author of study, said, “These results show the prediction of the diagnosis of primary hyperaldosteronism from the results of screening tests is not entirely accurate. Conduction of confirmatory tests is therefore required in all patients with a positive screening test.” The study was presented at the 29th Scientific Meeting of the European Society of Hypertension held June 21-24, 2019, in Milan, Italy.
Related Links:
University Hospital Olomouc and Palacký University
Gold Member
Flocked Fiber Swabs
Puritan® Patented HydraFlock®

Immunofluorescence Analyzer
IFA System

Electrolyte Analyzer
CBS-4000 (CBS-400)